Osteoporosis (means porous bone), one of the
metabolic disorders of bone is characterised by a
reduced bone mass with deterioration of the bone
micro architecture. It can predispose to fractures as
the fragile nature of the bone is often increased (1).
It is often considered as a “silent disease” as it
progresses rapidly without any appreciable symptoms
till a fracture occurs either spontaneously or
traumatically. It is also shown to have a marked public health burden due to its association with high
morbidity and mortality thereby increasing the
economic cost (2). The annual burden of osteoporosis
worldwide is around 200 million, of which the US
accounts for 1.5 million cases. The major economic
burden is due to vertebral and non-vertebral fractures
as they require a high expense to treat and often
have detrimental consequences. Following a hip
fracture, the risk of deaths is one in four in the
consecutive year (3).
WHO (Worl d Health Organisation) definition of
osteoporosis:
WHO has defined osteoporosis based on the
“measurement of bone mineral density (BMD) at
the hip or lumbar spine by dual energy X-ray
absorptiometry (DXA) and T-score” as shown in
Table I (4).

T-score is used for postmenopausal women and men > 50 years. A score of > -1.0 is normal, -1.0 to -2.5
as osteopenia (low bone m ass), > -2.5 as
osteoporosis and > -2.5 with one or more fractures
as severe or established osteoporosis (4).
However, to diagnose osteoporosis in children,
prem enopausal wom en and m en <50 years,
International Society for Clinical Densitometry (ISCD)
has recommended the usage of race or ethnic
adjusted Z-scores instead of T-scores (4).
Z-score:

Etiopathogenesis:
The etiology of osteoporosis is multifactorial, some
of which include the lifestyle factors, genetic,
gastrointestinal, haematological, rheumatologic and
neurological disorders and a few medications which
are shown in Table II (4).


To understand the pathogenesis of osteoporosis, an
aspect of bone remodelling (bone turnover) comes
into picture. It is the replacement of an old bone
with a new bone and includes four phases – bone
resorption, reversal, formation and mineralisation.
However, the main underlying factor is because of
an imbalance between bone formation and resorption
that can lead to fractures as shown in Fig. 1 (5).

Available treatment options for osteoporosis:
The treatment options available for osteoporosis
include the following –
1. Non-pharmacologic treatment:
- Lifestyle modifications: Calcium & Vitamin-D through diet
- Physical activity
- Smoking cessation; limited alcohol & caffeine
intake
2. Pharmacologic treatment:
a) Anti-resorptive drugs:
- Bisphosphonates (BP’s) – Alendronate,
Ibandronate, Zoledronate
- RANKL (receptor activator of NF-kβ ligand)
antibody – Denosumab
- Estrogen replacem ent – Conjugated
estrogens (CE)
- Selective estrogen receptor modulators
(SERM’s)–Raloxifene, Bazedoxifene
- Calcitonin
An outline of the mechanism of anti-resorptive
drugs, in general, is shown in Fig. 2.
b) Anabolic drugs: Parathyroid hormone (PTH)
peptides – Teriperatide (6)

Non-pharmacologic treatment:
Lifestyle modifications do have an impact on the
maintenance of bone health. Some of these include
adequate intake of calcium (1000–1200 mg/day) and
vitamin D (600-800 IU/day), weight bearing exercises
(at least 30 minutes/day), avoiding high alcohol intake
(> 2 servings/day), avoiding or quitting smoking,
decreasing intake of caffeine and by providing moral,
emotional and psychological support by health care
providers and family members. Meta-analyses were
performed in osteoporotic women who received
calcium and Vitamin-D supplementation. One of
these studies revealed that vitamin D alone was not
effective in reducing the risk of fractures. However,
another meta-analysis showed that there is a
decrease in the risk of fractures at both vertebral as
well as non-vertebral sites. Though the results are
often conflicting; overall, it was found that adequate
supplementation of calcium and vitamin-D can
promote bone health by preventing the bone loss to
a certain extent in osteoporotic patients (6).
Pharmacologic treatment:
Newer FDA (Food and Drug Administration) approved
drugs (2013 – 2017):
The drugs approved include - abaloparatide,
conjugated estrogens/bazedoxifene.
Abaloparatide: (ABL), (Brand name: Tymlos), 2017
It is a potent & selective synthetic analog of
parathyroid hormone related protein (PTHrP), 1-34
indicated to treat postmenopausal osteoporotic
women with high fracture risk. It is given as 80 µg
subcutaneously in the periumbilical region once daily
with a prefilled pen containing 30 doses. It causes
activation of the cyclic AMP signalling pathway in
target cells thereby exerting its anabolic effect on
bone. The most common ADR’s include orthostatic
hypotension, hypercalcemia, hypercalciuria,
urolithiasis and some others like headache, nausea,
dizziness, palpitations, vertigo, abdominal pain (7).
Preclinical studies: Abaloparatide (ABL) when given
at different doses of 5 and 20 µg/kg for 6 weeks
increased BMD in ovarectomised (OVX) rats in a
dose dependent manner. However, an evidence of
bone cancer (osteosarcoma) is seen on long term
usage, hence the label comes with black box warning
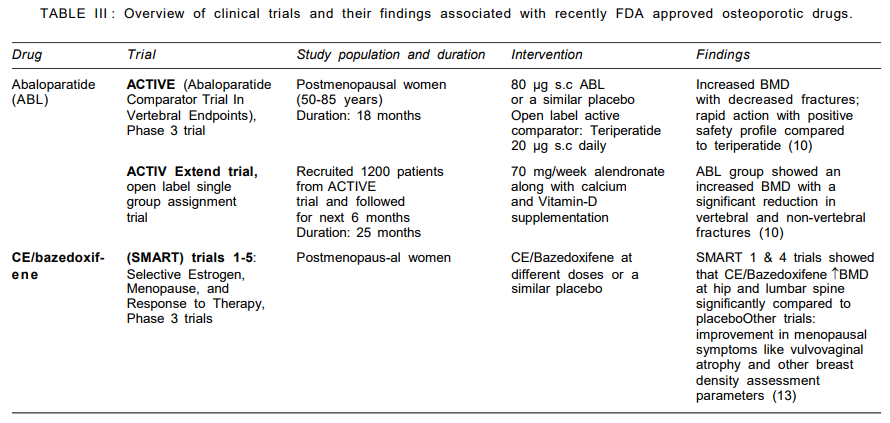
(8). Some of the clinical studies which had shown a
remarkable benefit with ABL are mentioned in Table
III below (10).
Conjugated estrogens (CE)/bazedoxifene, (Brand name:
Duavee), 2013
CE are extracted from the pregnant mares urine after
purification and blending with sodium salts.
Bazedoxifene is a selective estrogen receptor
modulator (SERM), acting both as an estrogen
agonist/antagonist. FDA has approved it for preventing
postmenopausal osteoporosis and to treat vasomotor
symptoms of menopause. Conjugated estrogen (CE)/
bazedoxifene is available at 0.45 mg/20 mg tablet
once daily. It acts by mimicking the favourable
effects of estrogens; but simultaneously blocks
estrogen in tissues where it might be harmful. Thus,
CE with bazedoxifeneexerts a composite effect which
is specific to each organ. The side effects include muscle spasms, oropharyngeal pain, dyspepsia,
nausea, diarrhea, abdominal pain, dizziness, neck
pain (11). Preclinical studies: In a study conducted
in OVX monkeys, up to 25 mg/kg/day of bazedoxifene
was given for 18 months; and it helped in preserving
the bone mass and its associated strength (12). The
major breakthrough clinical studies with CE/
bazedoxifene that led to its approval are listed in
Table III below (13).
FDA approved drugs from 1995–2012:
Denosumab (Brand name: Prolia, Xgeva), 2010
RANKL inhibitor was approved by FDA to treat
postmenopausal osteoporosis with fracture risk, in
men with non-metastatic prostatic cancer receiving
androgen deprivation therapy, and in breast cancer
women receiving adjuvant aromatase inhibitor therapy.
Normally, RANKL activates a receptor present on
osteoclasts called RANK that causes bone resorption;
denosumab acts by inhibiting this activation. It is
administered subcutaneously 60 mg every 6 months
in the arm or abdomen with a single use prefilled
syringe. Daily supplementation of calcium 1000 mg
and Vitamin-D 400 IU is advised routinely. The side
effects include musculoskeletal pain, dermatological
reactions, hypercholesterolemia and osteonecrosis
of the jaw (14).
Raloxifene hydrochloride, (Brand name: Evista), 2007
It is an estrogen agonist or antagonist (SERM)
indicated for the prevention and treatment of
osteoporosis in postmenopausal women and to
reduce their risk of invasive breast cancer. It acts
dually by activation of estrogenic pathways, and by
inhibiting them in tissues where it might be harmful.
It is administered as 60 mg tablet once daily. Side
effects include leg cramps, hot flushes, flu syndrome,
and peripheral edema (15).
Zoledronic acid, (Brand name: Reclast), 2007
A bisphosphonate compound indicated for the
prevention and treatment of postmenopausal
osteoporosis, glucocorticoid-induced osteoporosis, to
enhance the bone mass in osteoporotic men and to
treat Paget’s disease of bone (men and women). It
acts on farnesyl pyrophosphate synthase (enzyme
present on osteoclasts) and prevent bone resorption.
It is administered as an infusion of 5 mg in 100 mL
for a minimum period of 15 minutes along with routine
calcium and Vitamin-D supplementation. Adverse
reactions include renal impairment, atypical femoral
fractures and osteonecrosis of jaw (16).
Ibandronate, (Brand name: Boniva), 2005
A bisphosphonate indicated to treat postmenopausal osteoporosis. It acts on osteoclasts and inhibits bone
resorption. It is given as 3 mg intravenously every 3
months. ADRs include muscle, joint & bone pain,
osteonecrosis of the jaw, atypical femoral fractures (17).
Conjugated estrogens, (Brand name: Premarin), 2003
It is indicated for the prevention of postmenopausal
osteoporosis, to treat advanced androgen dependent
carcinoma of the prostate and in the treatment of
vulvar and vaginal atrophy. It acts by retarding
postmenopausal boneloss and is given 0.625 mg
daily or cyclical regimens (25 days on drug & 5
days off drug). ADRs include cardiovascular events,
breast cancer and venous thromboembolism (18).
Teriperatide, (Brand name: Forteo), 2002
A recombinant human parathyroid hormone analogue
(1-34) approved to treat postmenopausal osteoporotic
women with a high risk for fracture, in men with
primary or hypogonadal osteoporosis with high
fracture risk and glucocorticoid-induced osteoporosis.
It preferentially acts on osteoblasts over osteoclasts
by acting on cortical and trabecular surfaces
stimulating bone formation. It is given 20 µg
subcutaneously once daily. The adverse drug
reactions include arthralgia, urolithiasis and
orthostatic hypotension (19).
Estradiol transdermal patch, (Brand name: Alora), 2002
This patch is available at different doses like 0.025,
0.05, 0.075 and 0.1 mg of estradiol per day. The
reason behind the development of this patch is its
increased potency when compared to estrone and
estriol. The benefit of having a transdermal patch
over oral therapy is that – the target therapeutic
concentrations in plasma are attained at a lesser
dose by a patch. The BMD was markedly increased
in comparison to placebo when treated for two years
(20).
Other drugs approved for osteoporosis: (1995–2000)
These include Estradiol / Norethindrone acetate
tablets (Activella 1/0.5, 0.5/1), 2000; estradiol
transdermal patch, (Climara patch), 1999; Esterified
estrogens, (Estratab 0.3 mg), 1998; Raloxifene,
(Evista), 1997; Alendronate sodium, (Fosamax),
1995; Calcitonin-salmon nasal spray, (Miacalcin),
1995; CE/MPA tablets, (Prempo and Premphase),
1995.
Some of the important clinical trials with currently
approved FDA drugs (1995-2012) are listed in Table
IV.

Off-label drugs used for osteoporosis:
a) Calcitriol: It is asynthetic Vitamin-D analogue that
promotes calcium absorption. It was approved
by FDA for the management of hypocalcemia and
metabolic bone disease in renal dialysis patients
(4).
b) Genistein: Anisoflavone phytoestrogen marketed
and approved by FDA as a medical food
(‘Fosteum’, brand name). It acts by increasing
the osteoblastic factors like bone alkaline
phosphatases (B-ALP) and decreasing
osteoclastic factors like collagen C-telopeptide
(4, 27). Several clinical trials were conducted,
however, they revealed conflicting results. Some
trials had demonstrated an increase in bone
mineral density (at femoral neck) and B-ALP timedependently (28) and act as anti-resorptive agents
(29); and few others showed that it failed to
prevent bone loss or menopausal symptoms
(30). Also, it was found that its potency is
com paratively less when com pared to
bisphosphonates like risedronate (29)
c) Bisphosphonates: These include etidronate,
pamidronate and tiludronate which are approved
by FDA for treatment in Paget’s disease and
hypercalcemia of malignancy. However, their role
in osteoporosis needs to be established.
d) PTH(1-84): This is found to decrease the fracture
risk when administered at 100 µg/day. It was
approved in Europe and some other countries
but not yet by the FDA.
e) Sodium fluoride (NaF): Acts by revitalizing the
formation of new bone, however, its role in decreasing fracture risk is controversial and
conflicting.
f) Tibolone: Estrogen like agent which is tissue
specific and was approved by Europe to prevent
postmenopausal osteoporosis but not yet by FDA
(4).
Alternatives to treat osteoporosis:
Traditional methods are available for many centuries
for the treatment of bone loss and its associated
fracture risk by isolating the active compounds from
several plant parts like seeds, roots, leaves, flowers.
They act in different ways - they are a rich source
of calcium, act on the gastrointestinal tract and
promote calcium absorption or decrease the release
of pro-inflammatory cytokines that lead to bone loss.
The plant products which are found useful include:
a) Allium cepa and Allium sativum (stem-useful part),
act by decreasing bone resorption b) Cnidiummonnieri (Coumarins, fruit is found useful), act by decreasing
osteoclast formation c) Anemarrhenasphodeloides (rhizome) act by increasing bone formation d)
Curculigoorchioides (rhizome) act by increasing
osteoblast proliferation and decreasing bone
resorption. Fatty acid supplementation is also found
helpful in reducing bone loss and it acts by enhancing
calcium absorption and also causes down regulation
of osteoclastogenesis, pro-inflammatory cytokines
and prostaglandins. These include n-3 alpha linoleic
acid (Perilla oil), α-linoleic acid, linoleic acid
(Flaxseed oil, Hemp oil), omega-3 essential fatty
acids, docosahexanoic acid &eicosapentanoic acid
(Salmon oil), omega-3 essential fatty acids (Cod liver
oil) (5).
Recent developments: Drugs awaiting FDA approval:
a) Anti-resorptive agents:
- Cathepsin K inhibitors – ONO-5334,
Odanacatib
- Strontium ranelate
b) Anabolic agents:
- Anti-sclerostin antibodies – Romosozumab,
Blosozumab
c) Combination therapies:
- Anti-resorptive & anabolic agents – BP’s +
PTH, SERM’s + PTH
- Two antiresorptive agents – BP’s + HRT
(hormone replacement therapy), BP’s +
SERM’s
Among the above mentioned newer drugs awaiting
approval, anti- resorptive agents have shown to
increase the BMD and decrease the fracture risk.
However, anabolic agents and combination therapies
are only found to increase the BMD lacking clear
cut evidence regarding a decrease in fracture risk
(6).
Cathepsin K inhibitors:
Cathepsin is a lysosomal cysteine protease which
causes collagen degradation in different tissues.
There are different types of cathepsins like cathepsin
B, L, S, K. However, cathepsin K is specific to bone
whereas the other types of cathepsin degrade
collagen in tissues like skin and lung. The idea behind
developing this class of drugs started from a rare
disorder named pycnodysostosis which is autosomal
recessive. The patients suffering from this disorder
have a mutation in cathepsin K gene leading to an
increased bone mass. So, the cathepsin K inhibitors
prevented the adverse effects of collagen degradation
in tissues like bone. It also promotes bone formation
with the help of clastokines (secretory products of
osteoclasts) as shown in Fig. 2 (35).
Cathepsin K inhibitors act on osteoclasts of bone
thereby releasing clastokines which help in the
differentiation of osteoblasts and promote bone
formation. These drugs are under different phases of
clinical trial to develop them as a treatment strategy
for the treatment of osteoporosis; and some of which
are listed in Table V.

Strontium ranelate (Brand name: Protelos):
It was approved by European Medicines Agency
(EMA) to treat postmenopausal osteoporotic women
with a high risk of hip and vertebral fractures, and
intolerant to other pharmacological agents. Though the mechanism of how it acts is not completely
understood, it had a beneficial effect on bone
formation with mild anti-resorptive effect. It acts on
the calcium sensing receptors (CaSR) thereby
inhibiting the function of osteoclasts and promoting
the activity of osteoblasts increasing the BMD and
decreasing the fracture risk. It also has an indirect
action on proliferation and differentiation of
osteoblasts. Strontium replaces the calcium ions in
hydroxyappetite crystals and increasing the BMD.
The adverse reactions include myocardial infarction
and other cardiovascular events, venous
thromboembolism, gastrointestinal discomfort,
seizures. The EMA has made strict regulations
regarding its usage only in osteoporotic men or
women with high risk of fractures and prohibited in
those with heart or other circulatory problems as it
is associated with an increased risk of serious heart
attacks (6).
Anti-sclerostin antibodies:
Sclerostin, primarily produced by osteocytes is a
190-kDa glycoprotein encoded by SOST gene.
Canonical Wnt/β-catenin signalling pathway is an
important mediator in bone formation. Wnt interacts
with its lipoprotein receptor related protein, LRP5/6
and its co-receptor Frizzled resulting in activation of
Disheveled (Dvl), an intracellular protein which inhibits
glycogen synthase kinase 3β (GSK3β). This results
in the survival of β-catenin which is then translocated
into the nucleus thereby promoting gene transcription
as shown in Fig. 3. This leads to growth and
proliferation, maturation, differentiation, functioning and death of osteoblasts and chondrocytes (35).
Wnt binds to its receptor and helps in the movement
of intracellular -catenin into the nucleus thereby
regulating gene transcription and promoting bone
formation.
Abbreviations: LRP5/6 - lipoprotein receptor related
protein 5/6; Dvl - Disheveled; GSK3 - glycogen
synthase kinase 3
Sclerostin acts by inhibiting the Wnt/-catenin
signalling pathway thereby preventing the interaction
between Wnt and LRP5/6. The idea of developing
anti-sclerostin antibodies started after the occurrence
of two rare autosomal recessive disorders namely
sclerosteosis and van Buchem disease. These
disorders have a SOST gene mutation leading to
loss of sclerostin resulting in an increased bone mass
and decreased risk of fractures. Anti-sclerostin
antibodies bind to sclerotin and facilitate Wnt-LRP5/
6 interaction thereby activating the pathway (35).
The drugs in this class include romosozumab and
blosozumab.
Romosozumab
It is an anti-sclerostin antibody; the safety and
efficacy of which was demonstrated in a phase 3
trial, FRAME trial (Fracture Study in Postmenopausal
Women with Osteoporosis). The efficacy data is
shown in Table IV; and the most common adverse
reactions reported in this trial include cardiovascular
events, osteoarthritis, hyperostosis, osteonecrosis
of jaw, and atypical femoral fractures. The underlying
mechanism of romosozumab is attributed to the
increased bone formation and decreased bone
resorption (35).
Blosozumab:
Blosozumab, a humanised monoclonal antibody acts
similarly like romosozumab by increasing bone
formation and decreasing bone resorption (36). The
efficacy data is listed in Table IV. However, the exact
duration for which it has to be taken is not yet
understood and further studies are needed to
conclude its duration of action. In a phase 2 trial,
the serum markers associated with bone formation
declined within 3 months in the follow-up period and
completely returned to baseline by the end of one
year post-treatment. The adverse events reported
were almost the same in both the groups. These
results support the usage of blosozumab as an
anabolic agent in the treatment of osteoporosis (37).
However, the long term safety concern is a debate
and the company that developed this drug finds it
difficult to manufacture subcutaneous formulation of
this preparation. So, they again reverted its
development from phase 2 to phase 1 to carry on
with further investigations taking the necessary
concerns into account (36).
Some of the clinical trials linked with anti-sclerostin
antibodies are listed in Table VI.


